

Blood Flow Restriction Training for Post-Operative ACL: Fad or Feasible? Courtney Poist, SPT
by Courtney Poist
April 18, 2023
During my last semester of physical therapy school, I have had the opportunity to complete a literature review on a topic relevant to our clinical experiences as part of our research curriculum. While participating in my last clinical rotation at Physiolete, I have witnessed several young individuals begin their rehabilitation journey after ACL repair. While rehabilitating, some patients performed exercises while a blood flow restriction cuff was applied to their involved lower extremity. Although I have seen some individuals utilize this type of device while weight lifting in the gym, I had not yet seen it applied in a therapeutic setting. I decided to perform my literature review on the use of blood flow restriction training on individuals undergoing ACLR rehabilitation. By performing this research, I wanted to better understand the common protocols of BFR use and the therapeutic benefits that this tool may provide for these individuals.
Background:
One of the most common lower extremity musculoskeletal conditions is ACL injury, occurring at an astounding rate of approximately 250,000 cases per year in the world. The NCAA reports that ACL tears have increased at a rate of 1.3% each year over a 16 year period. Additionally claiming that each year there are more than 2,000 student athletes that suffer from ACL tear. With ACL reconstruction (ACLR) surgery, the primary concerns are quadriceps atrophy, inter-limb muscular asymmetry, and articular loading imbalances. All these deficits may lead to increased occurrence of reinjury, decreased lower extremity function, and prolonged rehabilitation for those wanting to return to sports activity. Blood Flow Restriction training, otherwise known as “BFR”, has been a trending modality in recent years, but has it been scientifically backed as an effective clinical tool within physical therapy clinics- especially for those rehabilitating from ACLR?
Evidence:
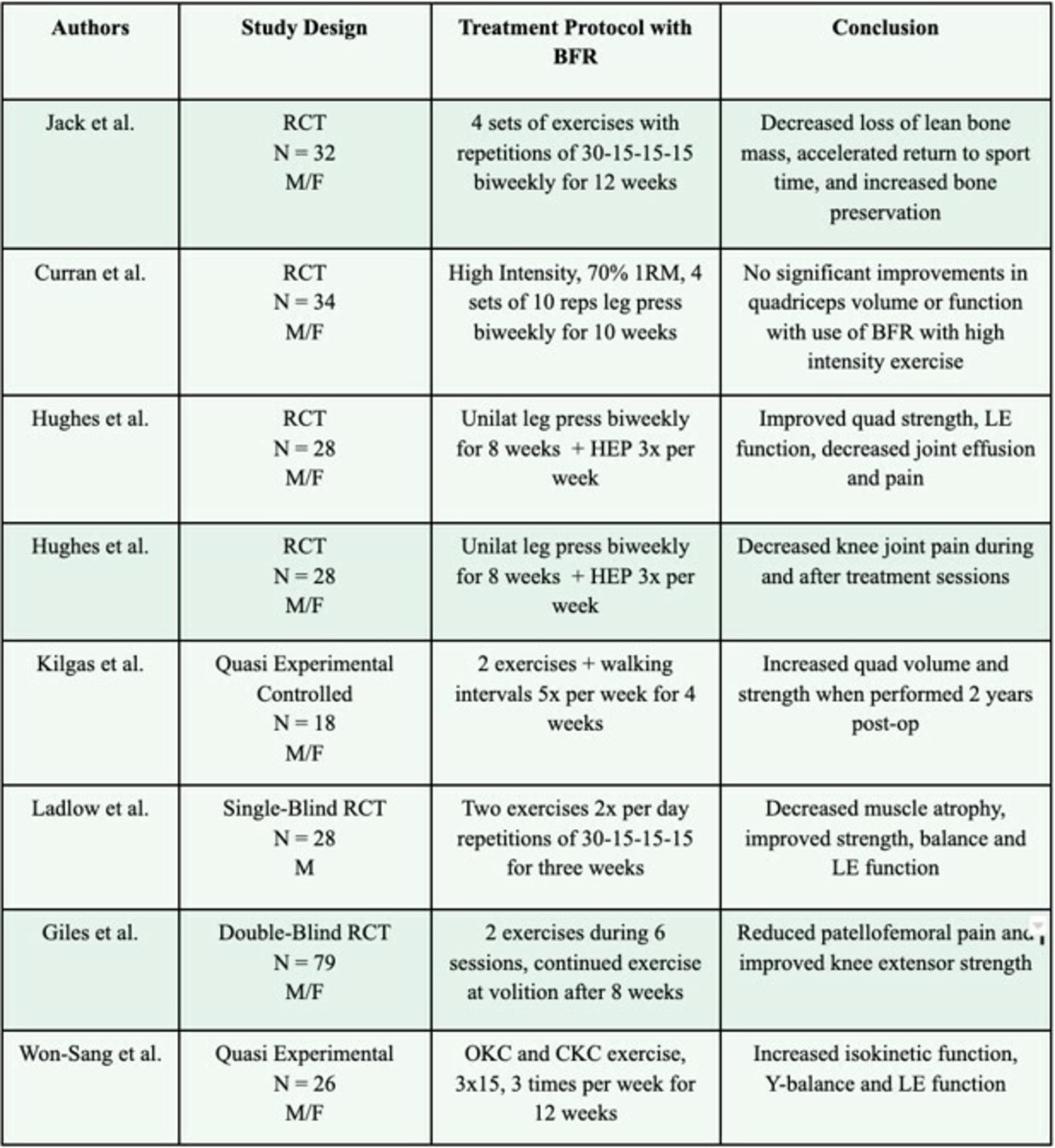
Conclusion:
For individuals undergoing ACLR Rehabilitation, the use of BFR can attenuate quadriceps atrophy, aid in knee extensor strength, and improve LE functional outcomes. It is also proven that the use of BFR can achieve similar strength gains as to high intensity, heavy loaded exercise all while decreasing intensity of knee pain and risk of re-injury. A novel finding of Jack et al. was that use of BFR within the first 12 weeks of ACL rehabilitation decreased the loss of lean bone mass, increased bone preservation and accelerated return to sport function. While reviewing these articles, I found that many clinicians implemented BFR at low intensities with high volume, utilizing a common rep schemes of 30-15-15-15. Most of the BFR cuffs within the studies were automatically inflated to calculate the level of occlusion pressure (LOP), and exercises were then performed with the cuff inflated to 80% of LOP. The type of exercises varied depending on phase of healing, however the majority of the exercises are targeted towards knee extensor and posterior chain strengthening. As research on BFR training on post-operative ACLR patients continues, treatment protocols should further standardize specificity, duration and frequency of exercises to yield the most optimal results.
Clinical Relevance:
BFR is a feasible clinical tool that can be implemented within the early phases of ACLR rehab. It is versatile and can be utilized without limiting exercise potential. As well as use of any other clinical modality, physical therapists must perform routine screenings and consider precautions and contraindications to BFR. Additionally, all patients should be educated on the risks and benefits of this modality and provide consent prior to the intervention. Although it is proven that BFR has positive effects, it is only practical if it is well tolerated by the patient.
References:
1. Astur DC, Xerez M, Rozas J, Debieux PV, Franciozi CE, Cohen M. Anterior cruciate ligament and meniscal injuries in sports: incidence, time of practice until injury, and limitations caused after trauma. Rev Bras Ortop. 2016;51(6):652-656. Published 2016 Jul 20. doi:10.1016/j.rboe.2016.04.008
2. NCAA.org. Obstacle course. NCAA.org. https://www.ncaa.org/news/2012/11/28/obstacle-course.aspx#:~:text=More%20than%202%2C000%20NCAA%20student,pre%2Dinjury%20levels%20of%20athleticism. Published June 14, 2016. Accessed April 16, 2023.
3. Jack RA 2nd, Lambert BS, Hedt CA, Delgado D, Goble H, McCulloch PC. Blood Flow Restriction Therapy Preserves Lower Extremity Bone and Muscle Mass After ACL Reconstruction [published online ahead of print, 2022 Jun 27].
4. Bobes Álvarez C, Issa-Khozouz Santamaría P, Fernández-Matías R, et al. Comparison of Blood Flow Restriction Training versus Non-Occlusive Training in Patients with Anterior Cruciate Ligament Reconstruction or Knee Osteoarthritis: A Systematic Review. J Clin Med. 2020;10(1):68. Published 2020 Dec 27. doi:10.3390/jcm10010068
5. Jack RA 2nd, Lambert BS, Hedt CA, Delgado D, Goble H, McCulloch PC. Blood Flow Restriction Therapy Preserves Lower Extremity Bone and Muscle Mass After ACL Reconstruction [published online ahead of print, 2022 Jun 27]. Sports Health. 2022;19417381221101006. doi:10.1177/19417381221101006
6. Curran MT, Bedi A, Mendias CL, Wojtys EM, Kujawa MV, Palmieri-Smith RM. Blood Flow Restriction Training Applied With High-Intensity Exercise Does Not Improve Quadriceps Muscle Function After Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. American Journal of Sports Medicine. 2020;48(4):825-837. Accessed March 18, 2023.
7. Grapar Zargi T, Drobnic M, Jkoder J, Strazar K, Kacin A. The effects of preconditioning with ischemic exercise on quadriceps femoris muscle atrophy following anterior cruciate ligament reconstruction: a quasi-randomized controlled trial. Eur J Phys Rehabil Med. 2016;52(3):310-320.
8. Hughes L, Rosenblatt B, Haddad F, et al. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post‐Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sports Medicine. 2019;49(11):1787-1805. doi:https://doi.org/10.1007/s40279-019-01137-2
9. Hughes L, Patterson SD, Haddad F, et al. Examination of the comfort and pain experienced with blood flow restriction training during post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: A UK National Health Service trial. Physical Therapy in Sport. 2019;39:90-98. doi:10.1016/j.ptsp.2019.06.014
10. Kilgas MA, Lytle LLM, Drum SN, Elmer SJ. Exercise with Blood Flow Restriction to Improve Quadriceps Function Long After ACL Reconstruction. Int J Sports Med. 2019;40(10):650-656. doi:10.1055/a-0961-1434
11. Iversen E, Røstad V, Larmo A. Intermittent blood flow restriction does not reduce atrophy following anterior cruciate ligament reconstruction. J Sport Health Sci. 2016;5(1):115-118. doi:10.1016/j.jshs.2014.12.005
12. Peter Ladlow, Russell J. Coppack, Shreshth Dharm-Datta, et al. Low-Load Resistance Training With Blood Flow Restriction Improves Clinical Outcomes in Musculoskeletal Rehabilitation: A Single-Blind Randomized Controlled Trial. Frontiers in Physiology 2018;9. Doi:10.338
13. Giles L, Webster KE, McClelland J, Cook JL. Quadriceps strengthening with and without blood flow restriction in the treatment of patellofemoral pain: a double-blind randomized trial. Br J Sports Med. 2017;51(23):1688-1694. doi:10.1136/bjsports-2016-096329
14. Won-Sang Jung, Seung-Hwan Kim, Sang-Seok Nam, Jeong-Weon Kim, Hwang-Woon Moon. Effects of Rehabilitation Exercise with Blood Flow Restriction after Anterior Cruciate Ligament Reconstruction. Applied Sciences. 2022;12(12058):12058. doi:10.3390/app122312058